LIKITHA’S ELOG
This is an online E log book to discuss our patient's de-identified health data shared after taking his/ her /guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Here is a case which I have seen:-
A 50 year old male patient came to the opd on 27/08/20.
Patient was apparently symptomatic 10 years back. Patient first went to the hospital with c/o fever, giddiness and sweating. Then local doctor observed high blood sugars and started on OHA 10 years back.
Later he had h/o trauma on 2nd toe of Rt LL 1 year back. Gradually his 3rd and 4th toes of Rt LL became gangrenous.
Then surgery was planned for dysarticulation and debridement of Rt 2,3,4th toes of Rt LL.
Then 4 months later, he had swelling over Rt lower limb (base of great toe) and gradually developed swelling and became gangrenous over 4 months to all over Rt fore foot.
Patient had high sugars during that period and patient consulted few doctors for swelling and sugar controls. Regular daily dressing was done by patient himself but as symptoms didn’t subside, patient underwent amputation 1 month back. Since 6 months, the patient developed multiple tiny itchy swellings that used to heal with scars (consulted few dermatologist and he was told that those lesions were due to high blood sugars)
6 months back patient developed localised swelling over left deltoid region ?Carbuncle and it was locally drained by a surgeon.
Patient also had recurrent swellings all over body 5 months back. He also had h/o carbuncle.
Patient gives history of pain abdomen associated with vomitings 1 year back and was diagnosed as pancreatitis. Conservative management was done.Chronic alcoholic since 20 years, 90ml whiskey/2days.


He is not a k/c/o asthma, TB, CAD, CVA, epilepsy.
GENERAL EXAMINATION-
Patient is conscious, coherent and cooperative.
Moderately built and nourished.
Vitals -
Temp- Afebrile
Bp- 160/110mmHg
PR- 78bpm
RR- 18cpm
Pallor +, icterus, cyanosis , clubbing, pedal edema, lymphadenopathy.
SYSTEMIC EXAMINATION
PER ABDOMEN-
Shape - scaphoid
Tenderness is present in epigastric region
No local rise of temperature
No palpable mass
No organomegaly
Hernial orifices free
Bowel sounds present
RS-
Position of trachea central
NVBS +
No wheeze
No adventitious breath sounds
CVS-
S1S2 heard
No murmurs
Apex beat not felt
CNS-
Higher mental functions intact.
All cranial nerves intact.
Sensory- intact
Motor - intact
No cerebellar signs
INVESTIGATIONS-
CUE-



PLBS-


Dermatology opinion:



ECG-

DIAGNOSIS:
?LADA WITH UNCONTROLLED SUGARS WITH NON PROLIFERATIVE DIABETIC RETINOPATHY, RIGHT DIABETIC FOOT WITH POST GILLES AMPUTATION.
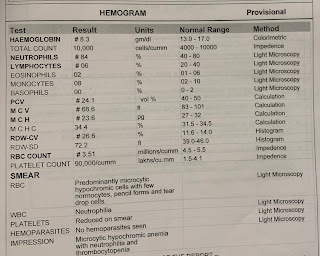
EARLY IRON DEFICIENCY ANEMIA
CHRONIC ALCOHOLIC SINCE 20 YEARS, HTN SINCE 5 YEARS.
Treatment:
Strict diabetic diet
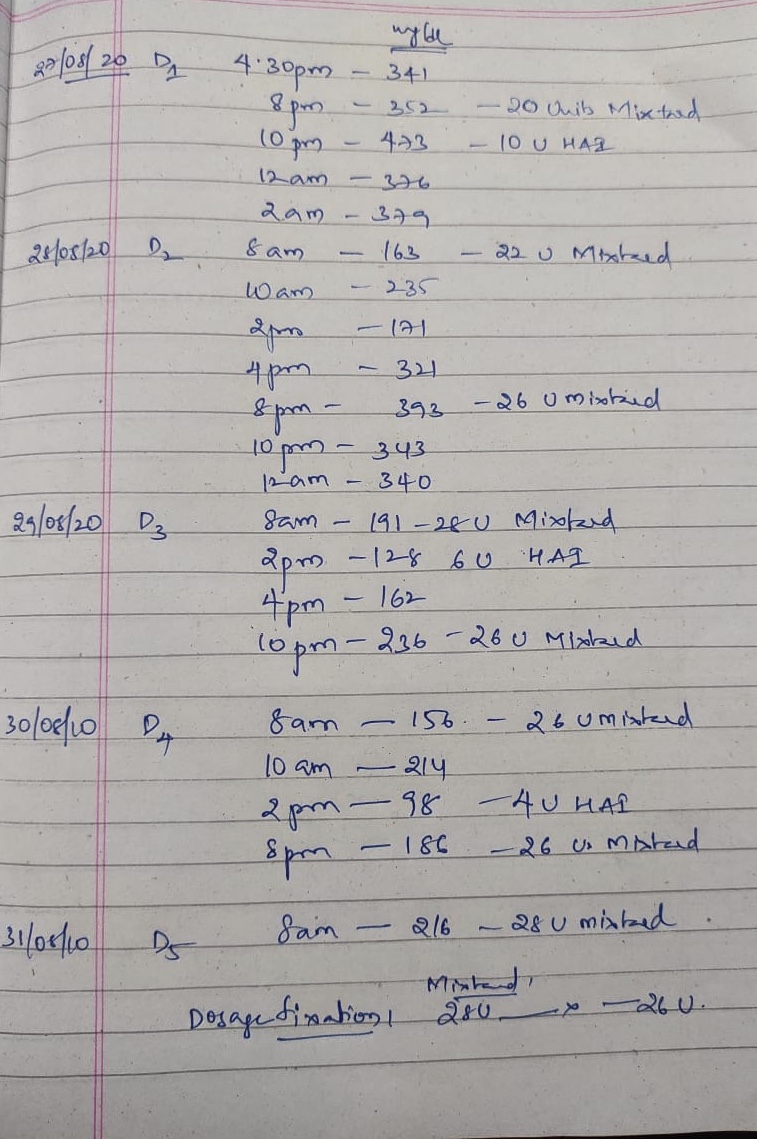
GRBS 8th hourly
TAB Amlong 5mg
Right foot elevation
Insulin Mixtard twice daily(28U-X-26U) along with insulin human actrapid (X-6U-X)
Tab Metformin 500mg PPO BD

Comments
Post a Comment